

health 2021


Previous work has specifically described the potential for using telemedicine in disasters and public health emergencies. No telemedicine program can be created overnight, but U.S. health systems that have already implemented telemedical innovations can leverage them for the response to Covid-19.
A central strategy for health care surge control is “forward triage” — the sorting of patients before they arrive in the emergency department (ED).
Direct-to-consumer (or on-demand) telemedicine, a 21st-century approach to forward triage that allows patients to be efficiently screened, is both patient-centered and conducive to self-quarantine, and it protects patients, clinicians, and the community from exposure. It can allow physicians and patients to communicate 24/7, using smartphones or webcam-enabled computers.
Respiratory symptoms — which may be early signs of Covid-19 — are among the conditions most commonly evaluated with this approach. Health care providers can easily obtain detailed travel and exposure histories. Automated screening algorithms can be built into the intake process, and local epidemiologic information can be used to standardize screening and practice patterns across providers.
Much medical decision making is cognitive, and telemedicine can provide rapid access to subspecialists who aren’t immediately available in person.
Recognizing that patients prioritize convenient and inexpensive care, Duffy and Lee recently asked whether in-person visits should become the second, third, or even last option for meeting patient needs
read the original article at https://www.nejm.org/doi/10.1056/NEJMp2003539
Lire l'article complet sur : www.nejm.org


Since the start of the pandemic, new technologies have been developed to help reduce the spread of the infection.
Some of the most common safety measures today include measuring a person’s temperature, covering your nose and mouth with a mask, contact tracing, disinfection, and social distancing. Many businesses have adopted various technologies, including those with artificial intelligence (AI) underneath, helping to adhere to the COVID-19 safety measures.
As an example, numerous airlines, hotels, subways, shopping malls, and other institutions are already using thermal cameras to measure an individual’s temperature before people are allowed entry. In its turn, public transport in France relies on AI-based surveillance cameras to monitor whether or not people are social-distancing or wearing masks. Another example is requiring the download of contact-tracing apps delivered by governments across the globe.
However, there are a number of issues.
While many of these solutions help to ensure that COVID-19 prevention practices are observed, many of them have flaws or limits. In this article, we will cover some of the issues creating obstacles for fighting the pandemic.
Issue #1. Manual temperature scanning is tricky
Issue #2. Monitoring crowds is even more complex
Issue #3. Contact tracing leads to privacy concerns
Issue #4. UV rays harm eyes and skin
Issue #5. UVC robots are extremely expensive
Issue #6. No integration, no compliance, no transparency
Regardless of the safety measures in place and existing issues, innovations are already playing a vital role in the fight against COVID-19. By improving on existing technology, we can make everyone safer as we all adjust to the new normal.
read the details at https://www.altoros.com/blog/whats-wrong-with-ai-tools-and-devices-preventing-covid-19/
Lire l'article complet sur : www.altoros.com

We developed and validated an accurate in-hospital mortality prediction score in a live EHR for automatic and continuous calculation using a novel model that improved upon SOFA.
The COVID-19 pandemic created an emergent need for a novel, accurate, and location and context-sensitive EHR-computable tool to predict mortality in hospitalized patients with and without COVID-19. Because developing a new score can take years, a predictive model must rely on well-validated scores.
In contrast, COVID-19 is a novel disease for which existing scores may be of limited but unknown predictive value.
As such, a predictive framework relying on multiple previously validated scores that can incorporate new information but only keeps the new inputs that explicitly improve performance is required. Stacked generalization provides a solution. A stacked model is built upon one or more baseline model(s) (e.g. SOFA) and incorporates additional models only when they improve prediction.
Materials and Methods
We developed, verified, and deployed a stacked generalization model to predict mortality using data available in the EHR by combining five previously validated scores and additional novel variables reported to be associated with COVID-19-specific mortality.
We verified the model with prospectively collected data from 12 hospitals in Colorado between March 2020 and July 2020. We compared the area under the receiver operator curve (AUROC) for the new model to the SOFA score and the Charlson Comorbidity Index.
Results
The prospective cohort included 27,296 encounters, of which 1,358 (5.0%) were positive for SARS-CoV-2, 4,494 (16.5%) required intensive care unit care, 1,480 (5.4%) required mechanical ventilation, and 717 (2.6%) ended in death. The Charlson Comorbidity Index and SOFA scores predicted mortality with an AUROC of 0.72 and 0.90, respectively. Our novel score predicted mortality with AUROC 0.94. In the subset of patients with COVID-19, the stacked model predicted mortality with AUROC 0.90, whereas SOFA had AUROC of 0.85.
Discussion
Stacked regression allows a flexible, updatable, live-implementable, ethically defensible predictive analytics tool for decision support that begins with validated models and includes only novel information that improves prediction.
read the paper abstract at https://academic.oup.com/jamia/advance-article/doi/10.1093/jamia/ocab100/6273353
read the entire paper at https://academic.oup.com/jamia/advance-article-pdf/doi/10.1093/jamia/ocab100/37905236/ocab100.pdf
Lire l'article complet sur : academic.oup.com
Identifying new COVID-19 cases is challenging. Not every suspected case undergoes testing, because testing kits and other equipment are limited in many parts of the world. Yet populations increasingly use the internet to manage both home and work life during the pandemic, giving researchers mediated connections to millions of people sheltering in place.
Objective: The goal of this study was to assess the feasibility of using an online news platform to recruit volunteers willing to report COVID-19–like symptoms and behaviors.
Methods: An online epidemiologic survey captured COVID-19–related symptoms and behaviors from individuals recruited through banner ads offered through Microsoft News. Respondents indicated whether they were experiencing symptoms, whether they received COVID-19 testing, and whether they traveled outside of their local area.
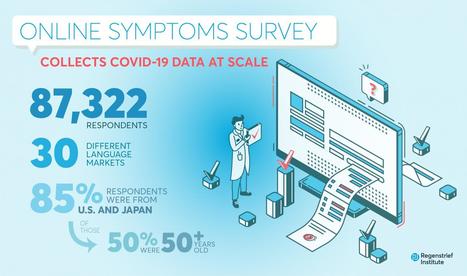
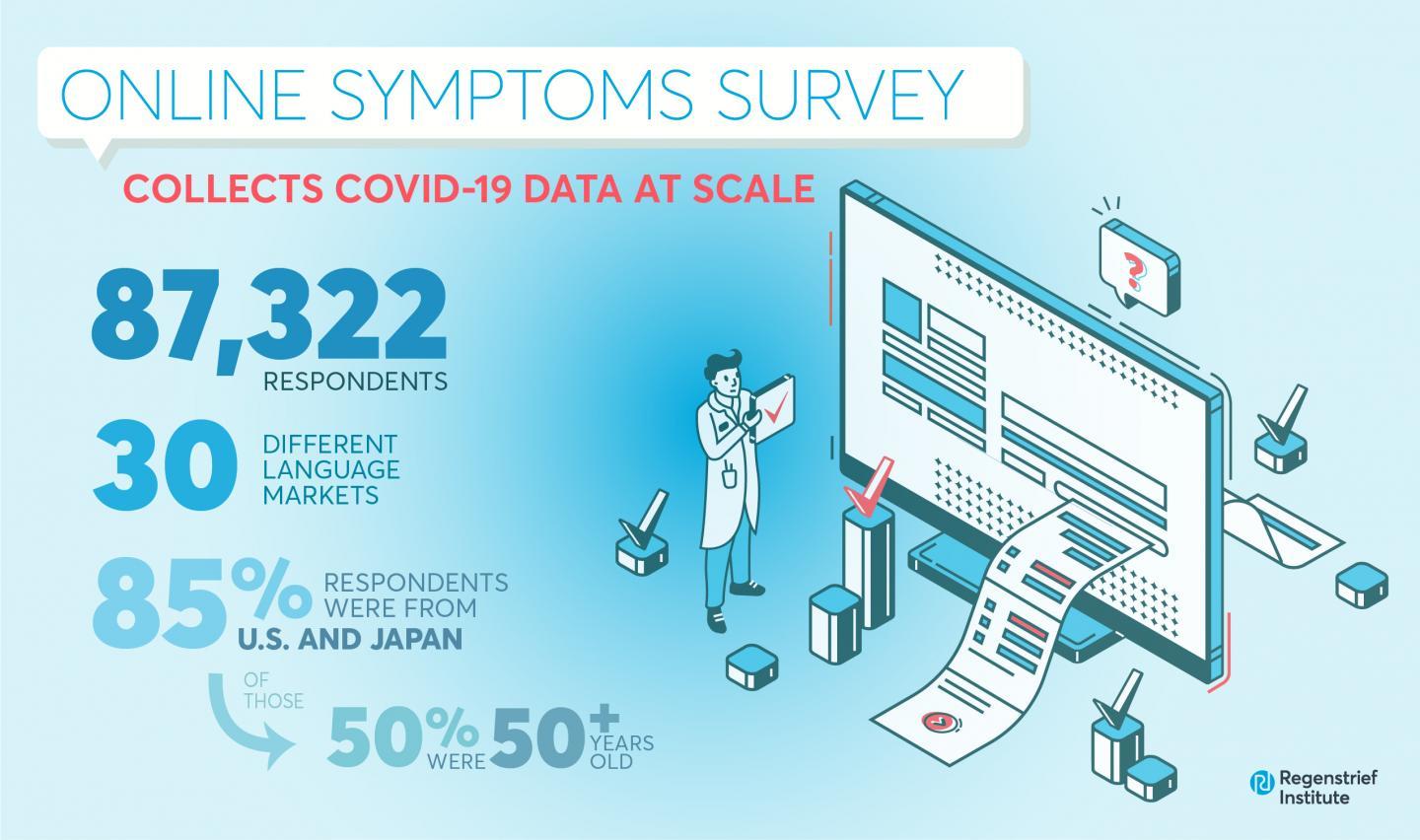
Results: A total of 87,322 respondents completed the survey across a 3-week span at the end of April 2020, with 54.3% of the responses from the United States and 32.0% from Japan. Of the total respondents, 19,631 (22.3%) reported at least one symptom associated with COVID-19. Nearly two-fifths of these respondents (39.1%) reported more than one COVID-19–like symptom. Individuals who reported being tested for COVID-19 were significantly more likely to report symptoms (47.7% vs 21.5%; P<.001). Symptom reporting rates positively correlated with per capita COVID-19 testing rates (R2=0.26; P<.001). Respondents were geographically diverse, with all states and most ZIP Codes represented. More than half of the respondents from both countries were older than 50 years of age.
Conclusions: News platforms can be used to quickly recruit study participants, enabling collection of infectious disease symptoms at scale and with populations that are older than those found through social media platforms. Such platforms could enable epidemiologists and researchers to quickly assess trends in emerging infections potentially before at-risk populations present to clinics and hospitals for testing and/or treatment.
source: Credit to Regenstrief Institute
read the entire study here : https://www.jmir.org/2021/5/e24742
Lire l'article complet sur : www.jmir.org